MSS 2021 SPRING ePOSTER
ISOLATED SPLENIC PELIOSIS: THE POTENTIAL FOR SPONTANEOUS RUPTURE AND THE ASSOCIATION WITH HEMATOLOGIC MALIGNANCY – A SINGLE-CENTER CASE SERIES
Michael LaRoque, Abhishek Chandra, Mason Nelson, Andrew Poffenberger, Michael Linden, George Nemanich, James V Harmon
Presenter: Michael LaRoque BS University of Minnesota
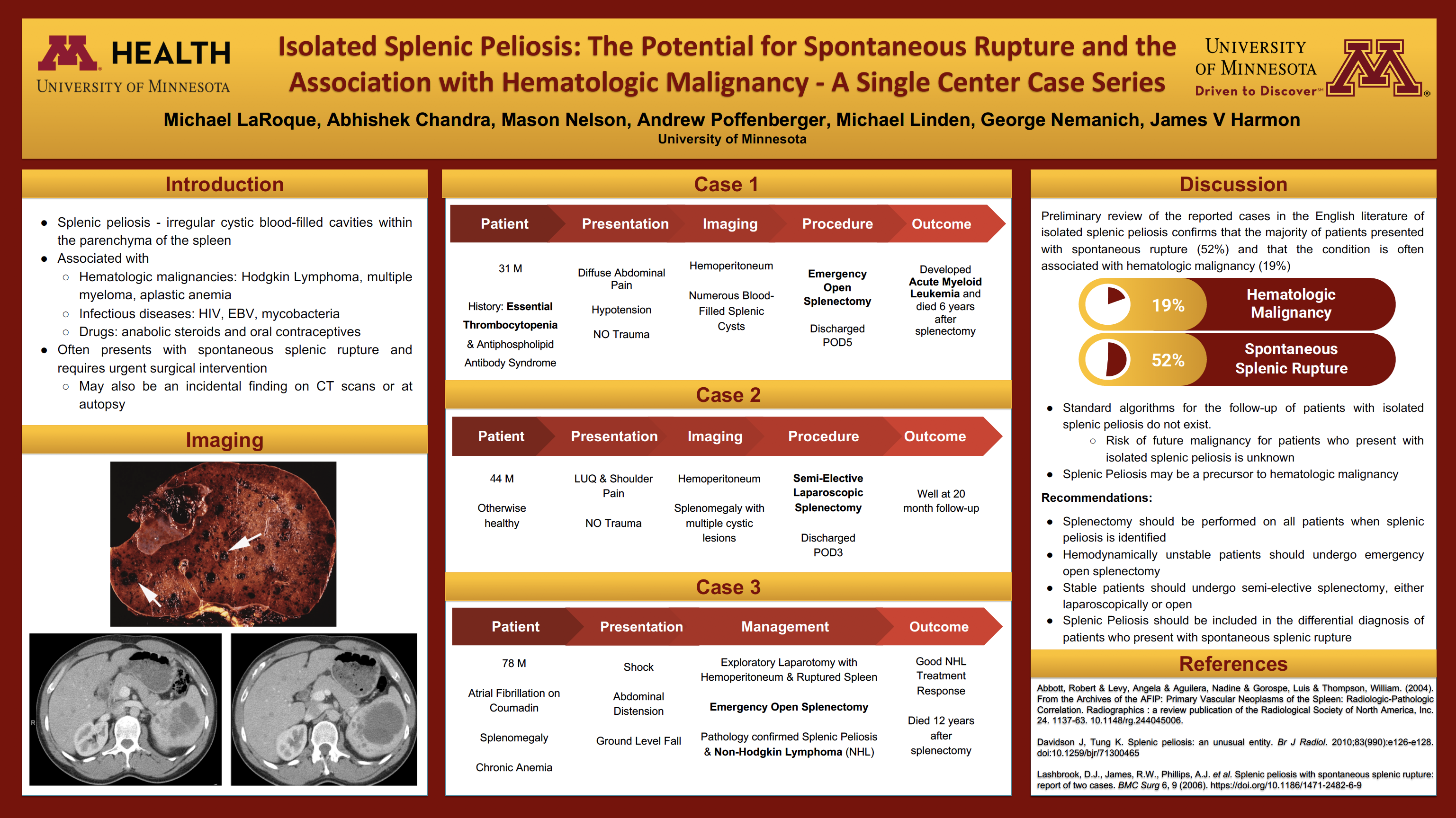
Introduction/Objective: Isolated splenic peliosis is an extremely rare condition with a potential for dramatic surgical presentation. Splenic peliosis often presents with spontaneous splenic rupture and requires urgent surgical intervention. However, the condition may also be recognized as an incidental finding on CT scans or at autopsy. Numerous associations with medications and other conditions have been described in the literature emphasizing the limited understanding of this condition. The focus of this case series is to draw attention to the surgical urgency required for this condition and to the potential association with hematologic malignancy.
Case Presentation: We present three patients with spontaneous splenic rupture due to isolated peliosis, one of which developed hematologic malignancy after initial presentation and one of which had a hematologic malignancy diagnosed during pathology review. One patient was managed laparoscopically.
Case 1: A 31 year-old man with a history of essential thrombocytopenia and antiphospholipid syndrome presented with worsening diffuse abdominal pain and severe hypotension. The patient denied trauma of any kind. A CT scan demonstrated hemoperitoneum and splenic rupture. The spleen was replaced with innumerable blood-filled cysts. Emergency open splenectomy with shed blood collection and reinfusion was performed without complication. The patient had an uneventful postoperative course and was discharged postoperative day 5. The patient died six years later from complications of AML.
Case 2: A 44 year-old otherwise healthy man presented with LUQ and shoulder pain with no reported trauma. A CT scan revealed an enlarged spleen with multiple splenic cystic lesions and free intraperitoneal fluid consistent with blood. A semi-elective laparoscopic splenectomy was performed, complicated by a small pancreatic leak which resolved after placement of a percutaneous drain and required no further intervention. The patient was discharged home on postoperative day 3. This patient was well at 20 months follow up.
Case 3: A 78 year-old man with atrial fibrillation on coumadin, known splenomegaly, and chronic anemia presented in shock with a massively distended abdomen. The patient had fallen from standing height, but denied other trauma. The patient was resuscitated with 2 units of PRBCs and taken urgently to the operating room. Exploratory laparotomy demonstrated 4 liters of intra-peritoneal blood and the spleen torn in two places. Open splenectomy was performed without complication. The patient required 6 units of PRBCs, 5 units of FFP, and 6 platelet units. Pathology confirmed a ruptured spleen, splenic peliosis, and Non-Hodgkin lymphoma (NHL). The patient had an excellent NHL treatment response, but died 12 years following splenectomy.
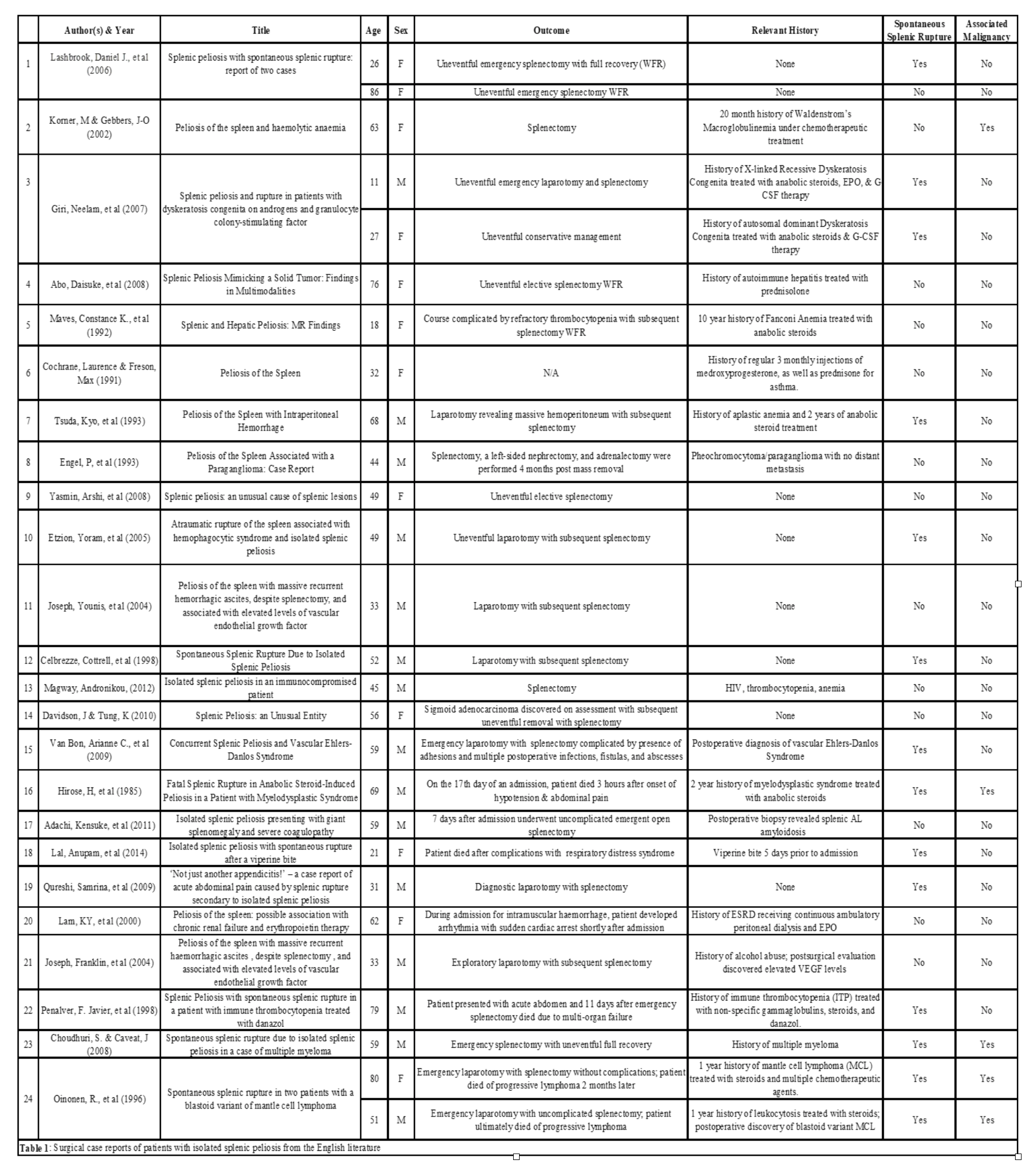
Discussion: The etiology of splenic peliosis remains unknown; however, the presentation to the surgeon may require urgent surgical intervention. The condition often exists without symptoms; however atraumatic splenic rupture has been well documented. Our preliminary review of the reported cases in the English literature of isolated splenic peliosis confirms that the majority of patients presented with spontaneous rupture (52%) and that the condition is often associated with hematologic malignancy (19%). See Table 1. Isolated splenic peliosis may present as an incidental CT finding, at autopsy, or as in our patients, with spontaneous rupture after minimal or no trauma.
Numerous reports of patients with splenic peliosis and associated hematologic disorders can be found in the literature. Warfel and Ellis reported in their 1982 review of splenic peliosis that 8 out of 12 patients had hematologic disorders including aplastic anemia, spherocytosis, myelofibrosis, myeloma, and Hodgkin disease. These associations have been further documented in the literature since.
Conclusion: We describe the presentation, management, and clinical outcome of three patients with spontaneous splenic rupture due to peliosis. Given that spontaneous rupture may result in fatal hemoperitoneum in patients with isolated splenic peliosis, we recommend splenectomy should be performed on all patients when splenic peliosis is identified. Hemodynamically unstable patients should undergo emergency open splenectomy. Stable patients should undergo semi-elective splenectomy, either laparoscopically or open. Standard algorithms for the follow-up of patients with isolated splenic peliosis do not exist. The risk of future malignancy for patients who present with isolated splenic peliosis is unknown.
{kind=link}
{kind=link}
{kind=link}